Patient Information Sheet
Enregistrer, Remplir les champs vides, Imprimer, Terminer!
How to create a Patient Information Sheet? Download this Patient Information Sheet template now!
Formats de fichiers gratuits disponibles:
.pdf- Ce document a été certifié par un professionnel
- 100% personnalisable
Business Entreprise insurance Assurance sheet drap Information Physical Physique Therapy Thérapie Sample Information Sheet Exemple de fiche d'information
Are you looking for a professional Patient Information Sheet? If you've been feeling stuck or lack motivation, download this template now!
Do you have an idea of what you want to draft, but you cannot find the exact words yet to write it down or lack the inspiration how to make it? If you've been feeling stuck, this Patient Information Sheet template can help you find inspiration and motivation. This Patient Information Sheet covers the most important topics that you are looking for and will help you to structure and communicate in a professional manner with those involved.
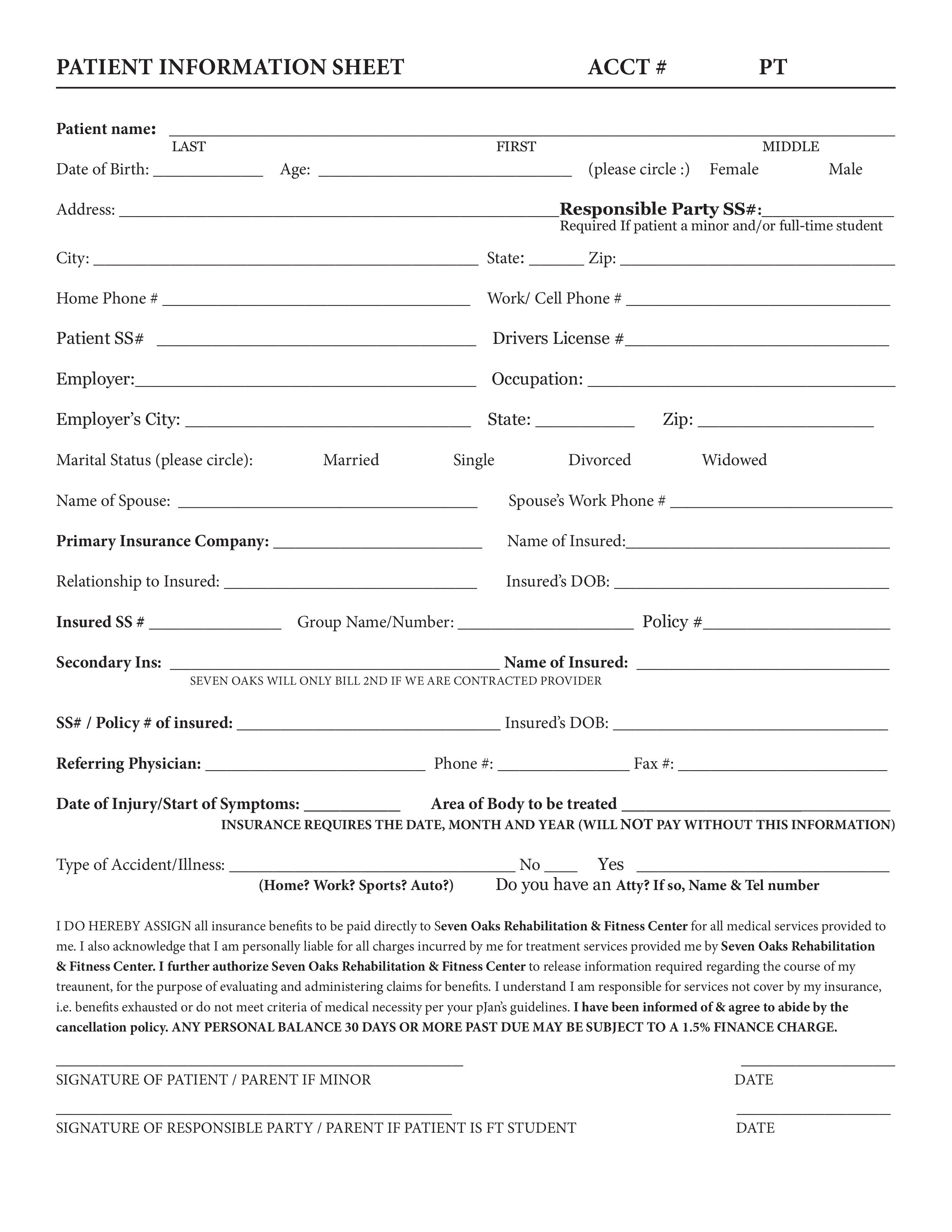
Patient Information Sheet ACCT PT Patient name: LAST FIRST MIDDLE Date of Birth: Age: (please circle :) Female Male Address: Responsible Party SS : Required If patient a minor and/or full-time student City: State: Zip: Home Phone Work/ Cell Phone Patient SS Drivers License Employer: Occupation: Employer’s City: State: Marital Status (please circle): Married Single Divorced Zip: Widowed Name of Spouse: Spouse’s Work Phone Primary Insurance Company: Name of Insured: Relationship to Insured: Insured’s DOB: Insured SS Group Name/Number: Policy Secondary Ins: Name of Insured: Seven Oaks will only bill 2nd if we are contracted provider SS / Policy of insured: Insured’s DOB: Referring Physician: Phone : Fax : Date of Injury/Start of Symptoms: Area of Body to be treated INSURANCE REQUIRES THE DATE, MONTH AND YEAR (WILL NOT PAY WITHOUT THIS INFORMATION) Type of Accident/Illness: No Yes (Home Work Sports Auto ) Do you have an Atty If so, Name Tel number I DO HEREBY ASSIGN all insurance benefits to be paid directly to Seven Oaks Re
Feel free to download this intuitive template that is available in several kinds of formats, or try any other of our basic or advanced templates, forms or documents. Don't reinvent the wheel every time you start something new...
Download this Patient Information Sheet template and save yourself time and efforts! You will see completing your task has never been simpler!
AVERTISSEMENT
Rien sur ce site ne doit être considéré comme un avis juridique et aucune relation avocat-client n'est établie.
Si vous avez des questions ou des commentaires, n'hésitez pas à les poster ci-dessous.