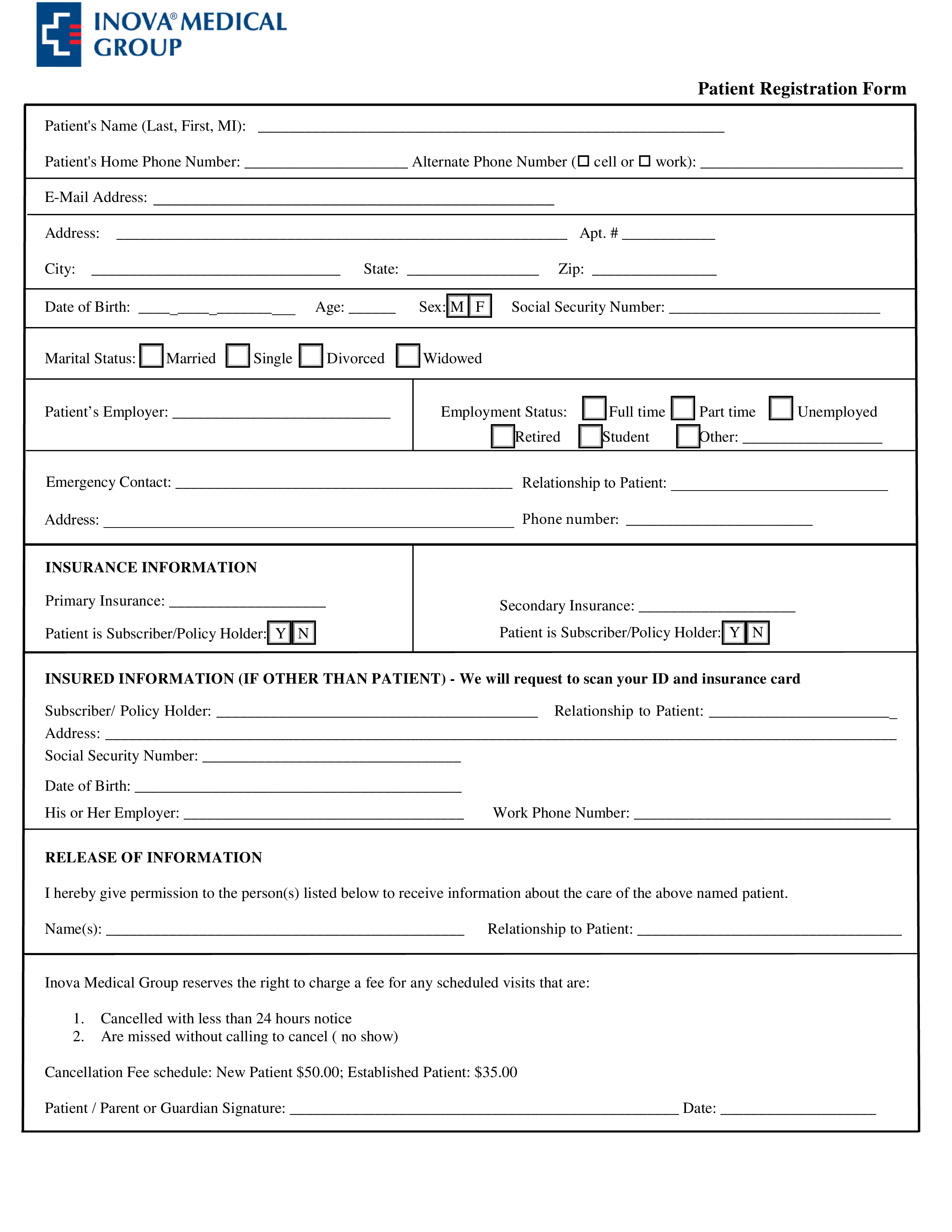
Printable Patient Registration Form
Speichern, ausfüllen, drucken, fertig!
How to create a Patient Registration Form? Download this Printable Patient Registration Form template now!
Verfügbare Gratis-Dateiformate:
.pdf- Dieses Dokument wurde von einem Professional zertifiziert
- 100% anpassbar
Business Unternehmen Health Gesundheit patient Patient Information Forms Formular Printable Registration Form Ausdruckbares Anmeldeformular Date Datum
Are you looking for a professional Printable Patient Registration Form? If you've been feeling stuck or lack motivation, download this template now!
Do you have an idea of what you want to draft, but you cannot find the exact words yet to write it down or lack the inspiration how to make it? If you've been feeling stuck, this Printable Patient Registration Form template can help you find inspiration and motivation. This Printable Patient Registration Form covers the most important topics that you are looking for and will help you to structure and communicate in a professional manner with those involved.
Cancelled with less than 24 hours notice Are missed without calling to cancel ( no show) Cancellation Fee schedule: New Patient 50.00 Established Patient: 35.00 Patient / Parent or Guardian Signature: Date:
Inova Medical Group HEALTH HISTORY Personal Information Date: Patient Name: Birth Date: // Age: Occupation Marital Status: Name of Partner/Spouse: Race: Asian Black or African American Native American White / Caucasian Other: Ethnicity: Do you identify with an Ethnic origin If yes, please note: Number of children: Children’s Names/Ages: Names/Specialties/Locations of Other Physicians Caring for You, including previous primary care doctor: Medical Information Please list any MEDICATIONS you are currently taking, prescribed or over the counter (use the back of the page if needed and indicate so): Medication Dosage Route Frequency Any Allergies to Medication or Food (list reactions): Preferred Pharmacy: Date of Last Complete Physical Exam: Date of Last Blood Work: Date of Last Colonoscopy: Date of Last Tetanus Shot: For Females: Date of Last Menstrual Period: Date of Last Pap Smear: History of Abnormal Pap (list date/s) Date of Last: Mammogram: DEXA: Number of Pregnancies: Miscarriages: Terminations: Liv
Feel free to download this intuitive template that is available in several kinds of formats, or try any other of our basic or advanced templates, forms or documents. Don't reinvent the wheel every time you start something new...
Download this Printable Patient Registration Form template and save yourself time and efforts! You will see completing your task has never been simpler!
HAFTUNGSAUSSCHLUSS
Nichts auf dieser Website gilt als Rechtsberatung und kein Mandatsverhältnis wird hergestellt.
Wenn Sie Fragen oder Anmerkungen haben, können Sie sie gerne unten veröffentlichen.