Medical Referral Form
Enregistrer, Remplir les champs vides, Imprimer, Terminer!
How to create a Medical Referral Form? Download this Medical Referral Form template now!
Formats de fichiers gratuits disponibles:
.pdf- Ce document a été certifié par un professionnel
- 100% personnalisable
Business Entreprise Health Santé form formulaire Client Forms Formulaire Taken Pris Date L'datte Referral Form Formulaire de référence Printable Referral Form Formulaire de référence imprimable Wic
How to write a Medical Referral Form? Download this Medical Referral Form template that will perfectly suit your needs.
Our collection of online health templates aims to make life easier for you. Our site is updated every day with new health and healthcare templates. By providing you this health Medical Referral Form template, we hope you can save precious time, cost and efforts and it will help you to reach the next level of success in your life, studies or work!
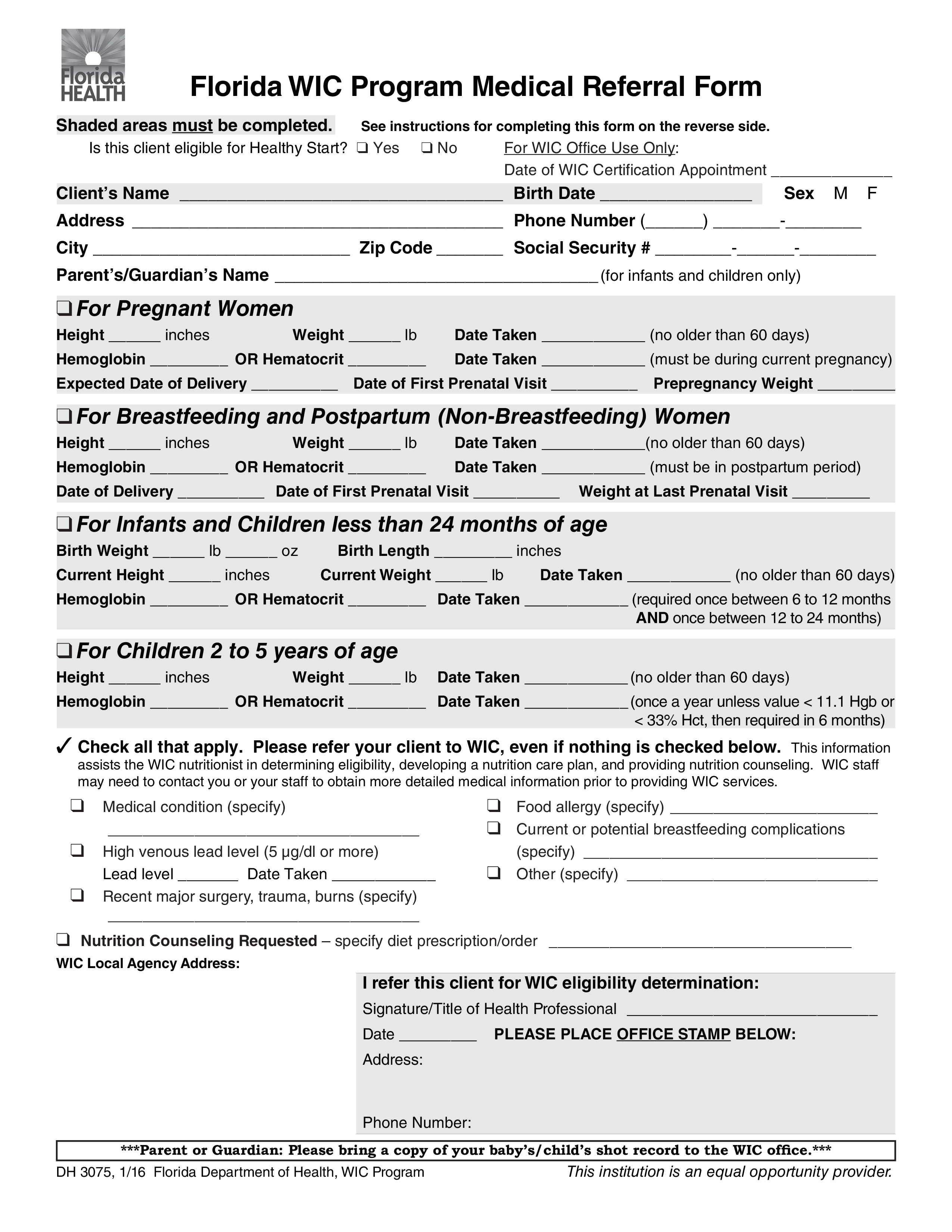
Is this client eligible for Healthy Start ❑ Yes ❑ No For WIC Office Use Only: Date of WIC Certification Appointment Client’s Name Birth Date Sex M F Address Phone Number () - City Zip Code Social Security -- Parent’s/Guardian’s Name (for infants and children only) ❑ For Pregnant Women Height inches Weight lb Hemoglobin OR Hematocrit Date Taken (no older than 60 days) Date Taken (must be during current pregnancy) Expected Date of Delivery Date of First Prenatal Visit Prepregnancy Weight ❑ For Breastfeeding and Postpartum (Non-Breastfeeding) Women Height inches Weight lb Hemoglobin OR Hematocrit Date Taken (no older than 60 days) Date Taken (must be in postpartum period) Date of Delivery Date of First Prenatal Visit Weight at Last Prenatal Visit ❑ For Infants and Children less than 24 months of age Birth Weight lb oz Current Height inches Birth Length inches Current Weight lb Date Taken (no older than 60 days) Hemoglobin OR Hematocrit Date Taken (required once between 6 to 12 months AND once between 12 to 24 months) ❑ For Children 2 to 5 years of age Height inches Weight lb Date Taken (no older than 60 days) Hemoglobin OR Hematocrit Date Taken (once a year unless value 11.1 Hgb or 33 Hct, then required in 6 months) ✓ Check all that apply..
This Medical Referral Form is intuitive, ready-to-use and structured in a smart way. Try it now and let this Medical Referral Form sample inspire you.
We certainly encourage you to download this Medical Referral Form now and use it to your advantage!
Also interested in other health and healthcare templates? AllBusinessTemplates is the most elaborate platform for downloading health templates and is updated every day with new health and healthcare related templates! Just search via our search bar or browse through our thousands of free and premium health forms and templates, contract, documents, letters, which are used by professionals in the healthcare industry. For example health care directive, mental health treatment plan, health management report, allergy log, healthy weekly meal plans, sick leave letter, health evaluation form, and much more...
AVERTISSEMENT
Rien sur ce site ne doit être considéré comme un avis juridique et aucune relation avocat-client n'est établie.
Si vous avez des questions ou des commentaires, n'hésitez pas à les poster ci-dessous.