Medical History Form
Enregistrer, Remplir les champs vides, Imprimer, Terminer!
How to create a Medical History Form? Download this Medical History Form template now!
Formats de fichiers gratuits disponibles:
.pdf- Ce document a été certifié par un professionnel
- 100% personnalisable
Business Entreprise Health Santé medical médical From De Dentist Dentiste Treatment Traitement Forms Formulaire Had Eu Printable Medical History Forms Formulaires d'histoire médicale imprimables
How to write a Medical History Form? Download this Medical History Form template that will perfectly suit your needs.
Our collection of online health templates aims to make life easier for you. Our site is updated every day with new health and healthcare templates. By providing you this health Medical History Form template, we hope you can save precious time, cost and efforts and it will help you to reach the next level of success in your life, studies or work!
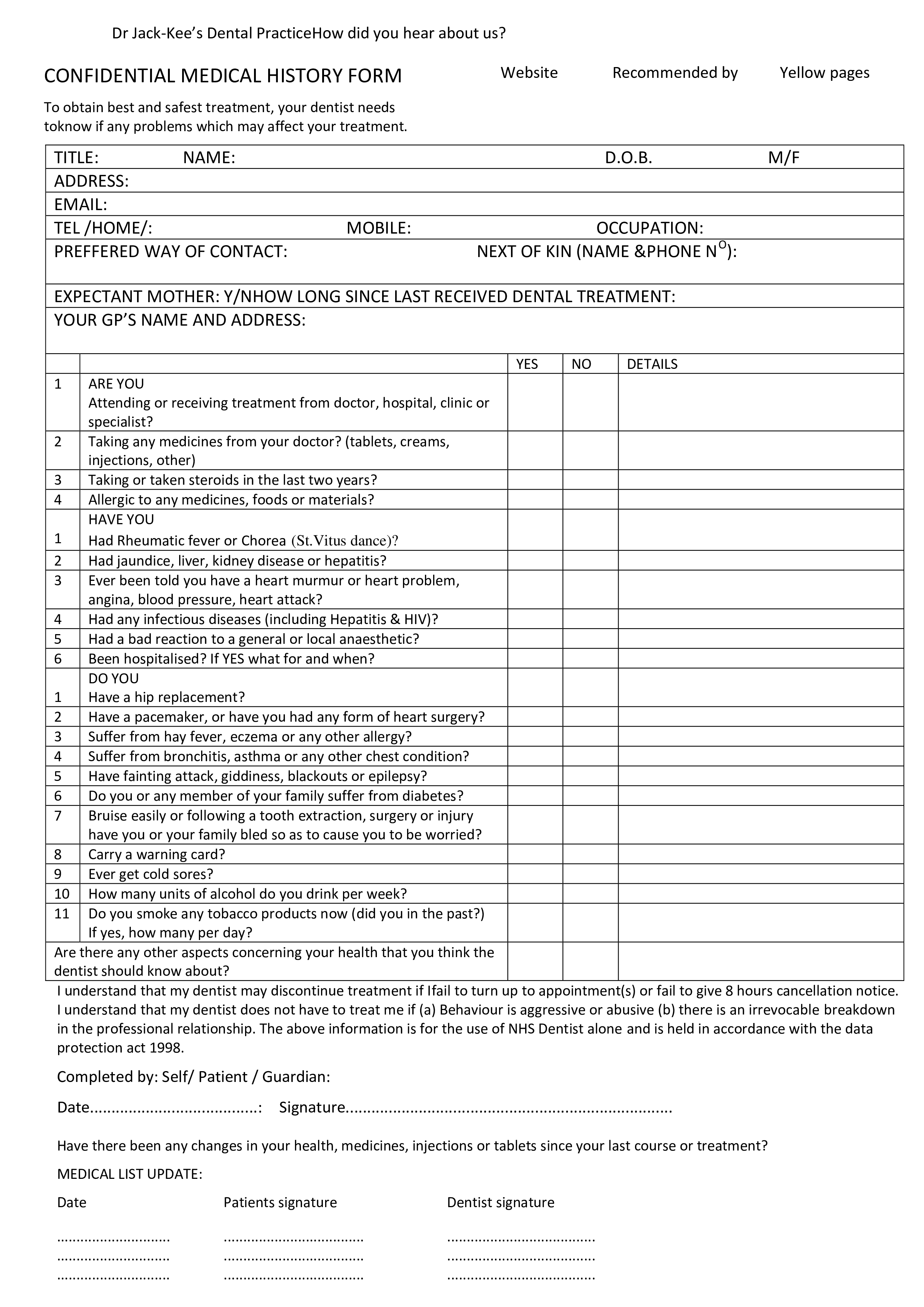
MOBILE: M/F OCCUPATION: NEXT OF KIN (NAME PHONE N O): EXPECTANT MOTHER: Y/NHOW LONG SINCE LAST RECEIVED DENTAL TREATMENT: YOUR GP’S NAME AND ADDRESS: YES NO DETAILS ARE YOU Attending or receiving treatment from doctor, hospital, clinic or specialist 2 Taking any medicines from your doctor (tablets, creams, injections, other) 3 Taking or taken steroids in the last two years 4 Allergic to any medicines, foods or materials HAVE YOU 1 Had Rheumatic fever or Chorea (St.Vitus dance) 2 Had jaundice, liver, kidney disease or hepatitis 3 Ever been told you have a heart murmur or heart problem, angina, blood pressure, heart attack 4 Had any infectious diseases (including Hepatitis HIV) 5 Had a bad reaction to a general or local anaesthetic 6 Been hospitalised If YES what for and when DO YOU 1 Have a hip replacement 2 Have a pacemaker, or have you had any form of heart surgery 3 Suffer from hay fever, eczema or any other allergy 4 Suffer from bronchitis, asthma or any other chest condition 5 Have fainting attack, giddiness, blackouts or epilepsy 6 Do you or any member of your family suffer from diabetes 7 Bruise easily or following a tooth extraction, surgery or injury have you or your family bled so as to cause you to be worried 8 Carry a warning card 9 Ever get cold sores 10 How many units of alcohol do you drink per week 11 Do you smoke any tobacco products now (did you in the past ) If yes, how many per day Are there any other aspects concerning your health that you think the dentist should know about I understand that my dentist may discontinue treatment if Ifail to turn up to appointment(s) or fail to give 8 hours cancellation notice..
This Medical History Form is intuitive, ready-to-use and structured in a smart way. Try it now and let this Medical History Form sample inspire you.
We certainly encourage you to download this Medical History Form now and use it to your advantage!
Also interested in other health and healthcare templates? AllBusinessTemplates is the most elaborate platform for downloading health templates and is updated every day with new health and healthcare related templates! Just search via our search bar or browse through our thousands of free and premium health forms and templates, contract, documents, letters, which are used by professionals in the healthcare industry. For example health care directive, mental health treatment plan, health management report, allergy log, healthy weekly meal plans, sick leave letter, health evaluation form, and much more...
AVERTISSEMENT
Rien sur ce site ne doit être considéré comme un avis juridique et aucune relation avocat-client n'est établie.
Si vous avez des questions ou des commentaires, n'hésitez pas à les poster ci-dessous.