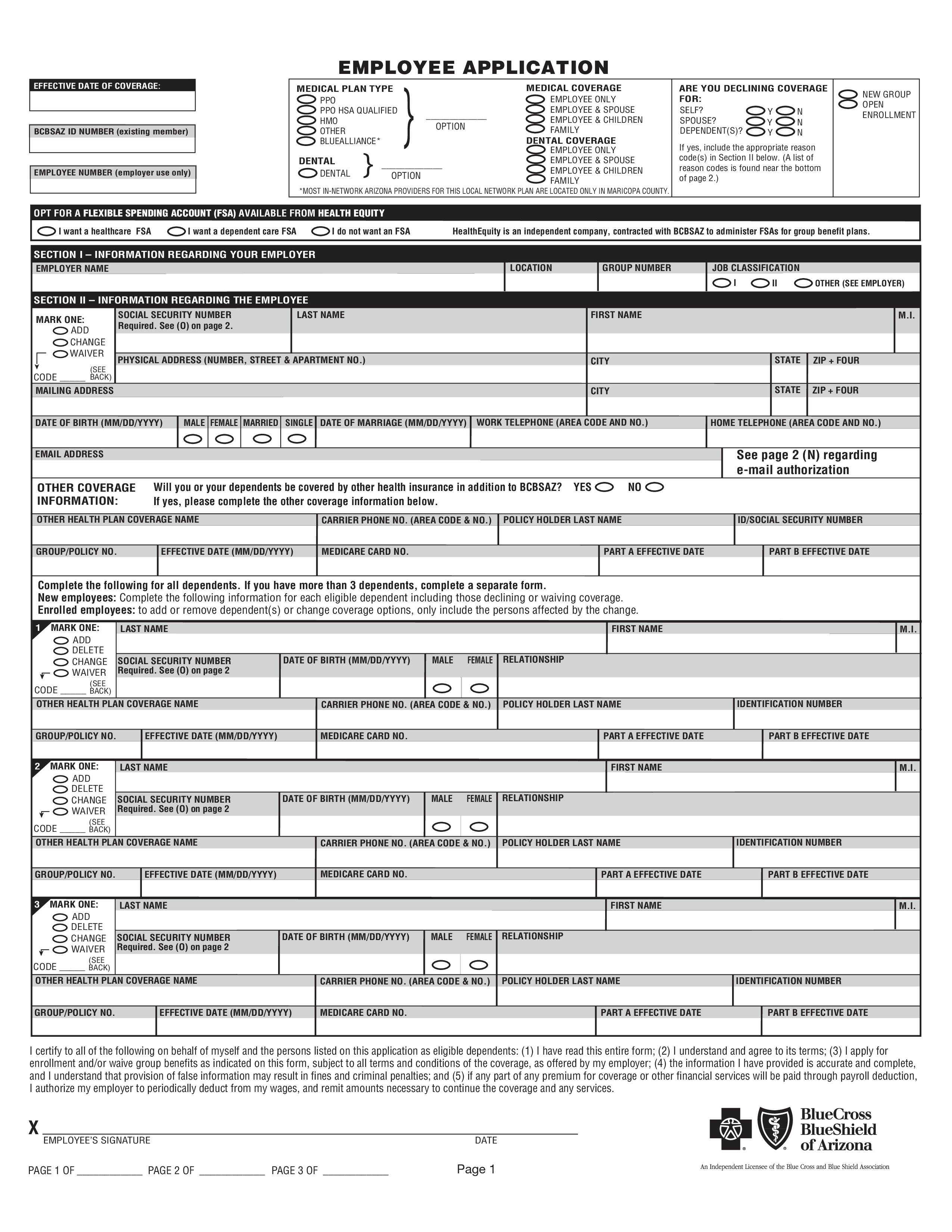
Blank Employee Application Sample
Guardar, completar los espacios en blanco, imprimir, listo!
How to create an employee Application Sample? Download this Blank Employee Application Sample template now!
Formatos de archivo disponibles:
.pdf- Este documento ha sido certificado por un profesionall
- 100% personalizable
Business Negocio HR RH employer empleador Group Grupo Date Fecha Coverage Cobertura
How to draft a Blank Employee Application Sample? Download this Blank Employee Application Sample template now!
We support you and your company by providing this Blank Employee Application Sample HR template, which will help you to make a perfect one! This will save you or your HR department time, cost and efforts and help you to reach the next level of success in your work and business!
This Blank Employee Application Sample has ways to grab your reader’s attention. It is drafted by HR professionals, intelligently structured and easy-to-navigate through. Pay close attention to the most downloaded HR templates that fit your needs.
Download this Human Resources Blank Employee Application Sample template now!
EMPLOYEE APPLICATION EFFECTIVE DATE OF COVERAGE: MEDICAL PLAN TYPE PPO PPO HSA QUALIFIED HMO OTHER BLUEALLIANCE BCBSAZ ID NUMBER (existing member) DENTAL DENTAL EMPLOYEE NUMBER (employer use only) _____________ OPTION _____________ OPTION MEDICAL COVERAGE EMPLOYEE ONLY EMPLOYEE SPOUSE EMPLOYEE CHILDREN FAMILY DENTAL COVERAGE EMPLOYEE ONLY EMPLOYEE SPOUSE EMPLOYEE CHILDREN FAMILY ARE YOU DECLINING COVERAGE FOR: SELF Y N SPOUSE Y N DEPENDENT(S) Y N NEW GROUP OPEN ENROLLMENT If yes, include the appropriate reason code(s) in Section II below.. POLICY HOLDER LAST NAME PART A EFFECTIVE DATE IDENTIFICATION NUMBER PART B EFFECTIVE DATE I certify to all of the following on behalf of myself and the persons listed on this application as eligible dependents: (1) I have read this entire form (2) I understand and agree to its terms (3) I apply for enrollment and/or waive group benefits as indicated on this form, subject to all terms and conditions of the coverage, as offered by my employer (4) the information I have provided is accurate and complete, and I understand that provision of false information may result in fines and criminal penalties and (5) if any part of any premium for coverage or other financial services will be paid through payroll deduction, I authorize my employer to periodically deduct from my wages, and remit amounts necessary to continue the coverage and any services..
Also interested in other HR templates? Browse through our database and have instant access to hundreds of free and premium HR documents, HR forms, HR agreements, etc
DESCARGO DE RESPONSABILIDAD
Nada en este sitio se considerará asesoramiento legal y no se establece una relación abogado-cliente.
Deja una respuesta. Si tiene preguntas o comentarios, puede colocarlos a continuación.