Client intake formulier
Opslaan, invullen, afdrukken, klaar!
De beste manier om een Client intake formulier te maken? Check direct dit professionele Client intake formulier template!
Beschikbare bestandsformaten:
.pdf- Gevalideerd door een professional
- 100% aanpasbaar
- Taal: English
- Digitale download (34.23 kB)
- Na betaling ontvangt u direct de download link
- We raden aan dit bestand op uw computer te downloaden.
Zakelijk medisch Van moeten Formulieren Intakeformulier Eenvoudig intake formulier
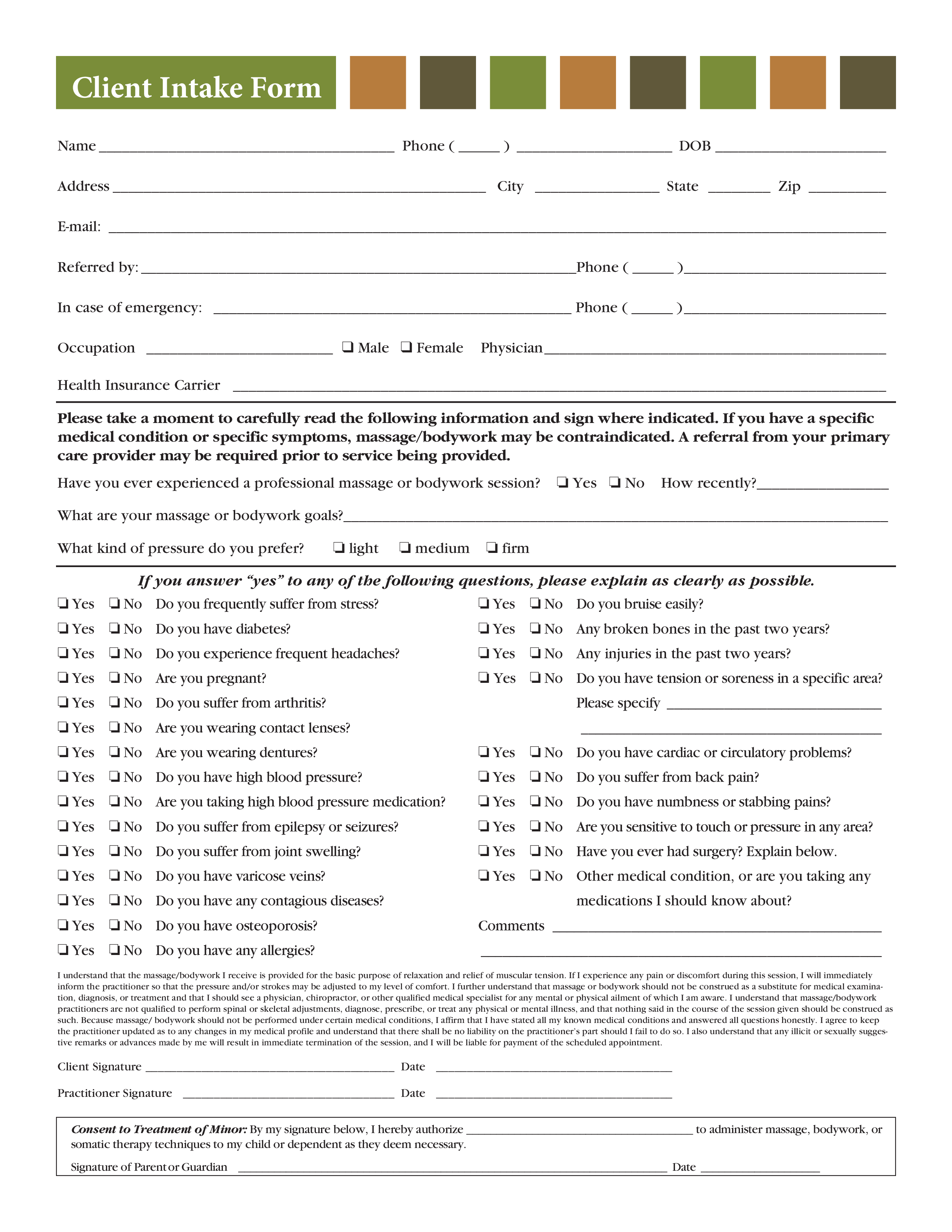
How to draft a Client Intake Form? An easy way to start completing your document is to download this Client Intake Form template now!
Every day brings new projects, emails, documents, and task lists, and often it is not that different from the work you have done before. Many of our day-to-day tasks are similar to something we have done before. Don't reinvent the wheel every time you start to work on something new!
Instead, we provide this standardized Client Intake Form template with text and formatting as a starting point to help professionalize the way you are working. Our private, business and legal document templates are regularly screened by professionals. If time or quality is of the essence, this ready-made template can help you to save time and to focus on the topics that really matter!
Using this document template guarantees you will save time, cost and efforts! It comes in Microsoft Office format, is ready to be tailored to your personal needs. Completing your document has never been easier!
Download this Client Intake Form template now for your own benefit!
Client Intake Form Name Phone ( ) DOB Address City State Zip E-mail: Referred by: Phone ( ) In case of emergency: Phone ( ) Occupation K Male K Female Physician Health Insurance Carrier Please take a moment to carefully read the following information and sign where indicated.. J Yes J No Do you frequently suffer from stress J Yes J No Do you bruise easily J Yes J No Do you have diabetes J Yes J No Any broken bones in the past two years J Yes J No Do you experience frequent headaches J Yes J No Any injuries in the past two years J Yes J No Are you pregnant J Yes J No Do you have tension or soreness in a specific area J Yes J No Do you suffer from arthritis J Yes J No Are you wearing contact lenses Please specify J Yes J No Are you wearing dentures J Yes J No Do you have cardiac or circulatory problems J Yes J No Do you have high blood pressure J Yes J No Do you suffer from back pain J Yes J No Are you taking high blood pressure medication J Yes J No Do you have numbness or stabbing pains J Yes J No Do you suffer from epilepsy or seizures J Yes J No Are you sensitive to touch or pressure in any area J Yes J No Do you suffer from joint swelling J Yes J No Have you ever had surgery Explain below..
DISCLAIMER
Hoewel all content met de grootste zorg is gecreërd, kan niets op deze pagina direct worden aangenomen als juridisch advies, noch is er een advocaat-client relatie van toepassing.
Laat een antwoord achter. Als u nog vragen of opmerkingen hebt, kunt u deze hieronder plaatsen.