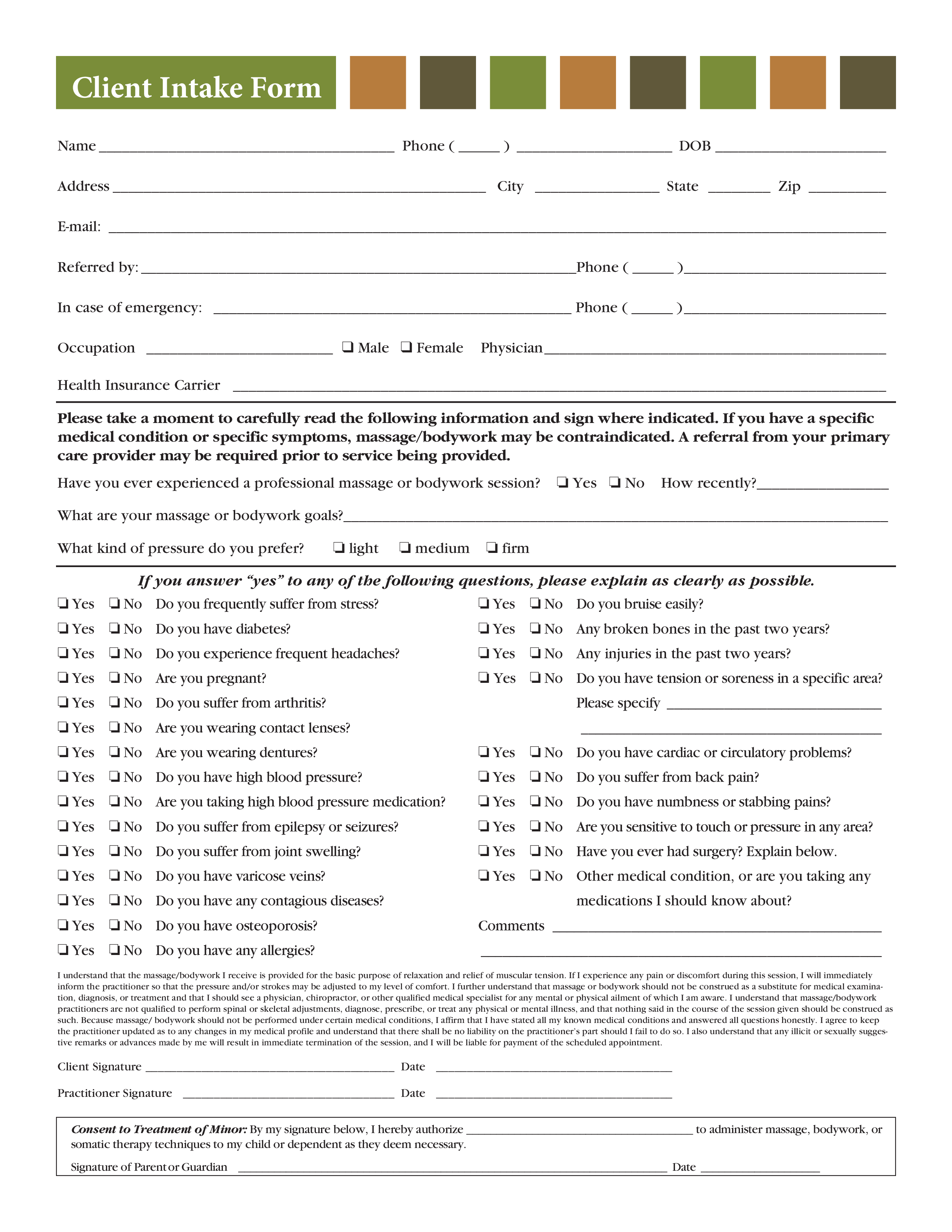
Client Intake Form
Enregistrer, Remplir les champs vides, Imprimer, Terminer!
How to create a Client Intake Form? Download this Client Intake Form template now!
Formats de fichiers gratuits disponibles:
.pdf- Ce document a été certifié par un professionnel
- 100% personnalisable
Business Entreprise medical médical From De Should Devrait Forms Formulaire Intake Form Formulaire d'admission Simple Intake Form Formulaire d'admission simple Massage
How to draft a Client Intake Form? An easy way to start completing your document is to download this Client Intake Form template now!
Every day brings new projects, emails, documents, and task lists, and often it is not that different from the work you have done before. Many of our day-to-day tasks are similar to something we have done before. Don't reinvent the wheel every time you start to work on something new!
Instead, we provide this standardized Client Intake Form template with text and formatting as a starting point to help professionalize the way you are working. Our private, business and legal document templates are regularly screened by professionals. If time or quality is of the essence, this ready-made template can help you to save time and to focus on the topics that really matter!
Using this document template guarantees you will save time, cost and efforts! It comes in Microsoft Office format, is ready to be tailored to your personal needs. Completing your document has never been easier!
Download this Client Intake Form template now for your own benefit!
Client Intake Form Name Phone ( ) DOB Address City State Zip E-mail: Referred by: Phone ( ) In case of emergency: Phone ( ) Occupation K Male K Female Physician Health Insurance Carrier Please take a moment to carefully read the following information and sign where indicated.. J Yes J No Do you frequently suffer from stress J Yes J No Do you bruise easily J Yes J No Do you have diabetes J Yes J No Any broken bones in the past two years J Yes J No Do you experience frequent headaches J Yes J No Any injuries in the past two years J Yes J No Are you pregnant J Yes J No Do you have tension or soreness in a specific area J Yes J No Do you suffer from arthritis J Yes J No Are you wearing contact lenses Please specify J Yes J No Are you wearing dentures J Yes J No Do you have cardiac or circulatory problems J Yes J No Do you have high blood pressure J Yes J No Do you suffer from back pain J Yes J No Are you taking high blood pressure medication J Yes J No Do you have numbness or stabbing pains J Yes J No Do you suffer from epilepsy or seizures J Yes J No Are you sensitive to touch or pressure in any area J Yes J No Do you suffer from joint swelling J Yes J No Have you ever had surgery Explain below..
AVERTISSEMENT
Rien sur ce site ne doit être considéré comme un avis juridique et aucune relation avocat-client n'est établie.
Si vous avez des questions ou des commentaires, n'hésitez pas à les poster ci-dessous.