HTML Preview Medical Expense Receipt page number 1.
English/英語
患者氏名 :
患者 ID :
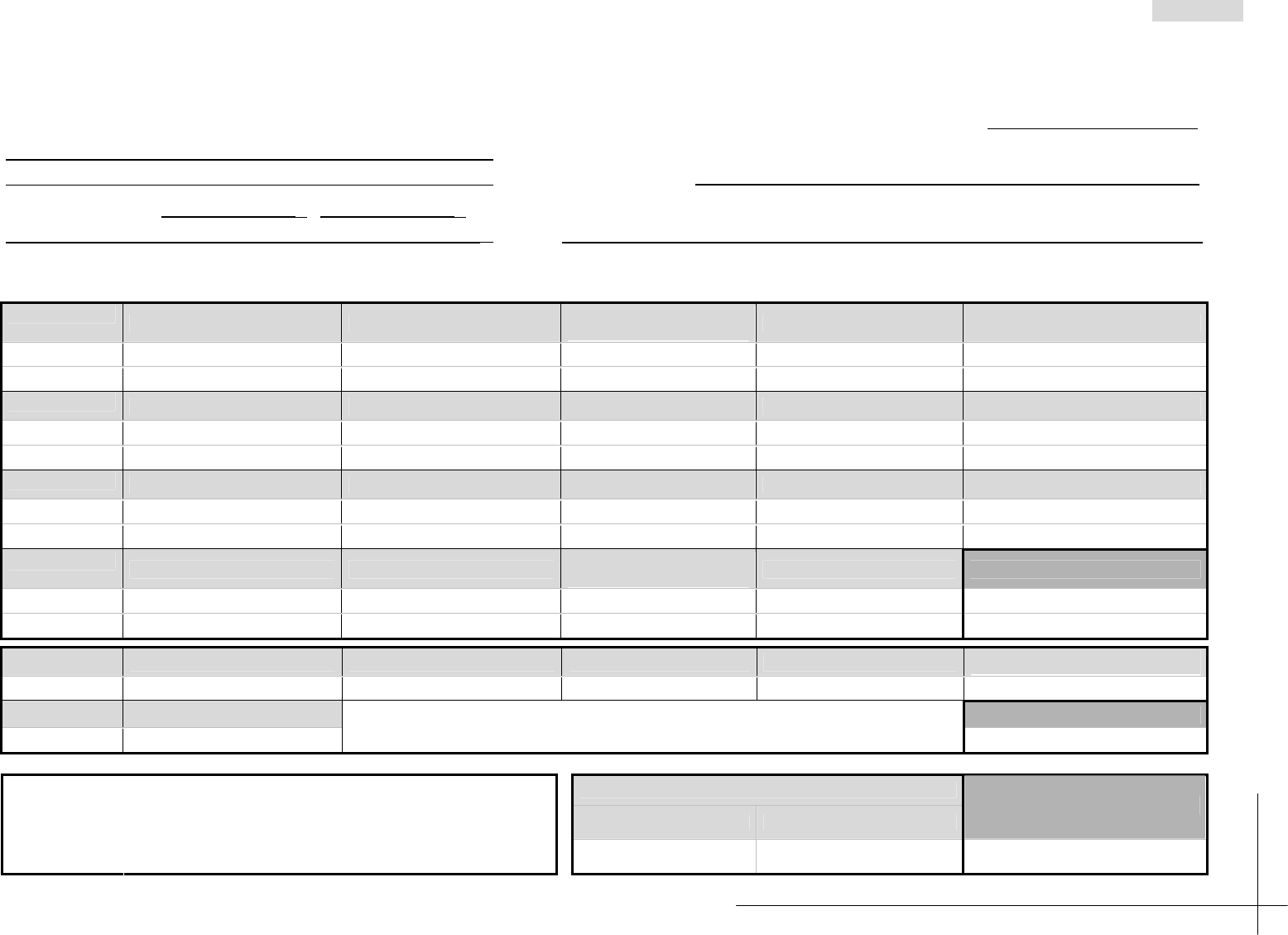
Medical Expense Receipt
Date issued (YYYY/MM/DD) : / /
Hospital name: □Outpatient □Inpatient □Second opinion
Department: Insurance type: (Percentage of patient liability: %)
Billing period: From / / to / /
Hospital ID No.: Patient name:
Sales tax
Subtotal to be taxed Tax
TOTAL RECEIVED
Comments:
¥ ¥
¥
Dietary therapy Documentation Delivery charges Extra room charges
Special or specified medical care
Patient liability
¥ ¥ ¥ ¥ ¥
Others SUBTOTAL
Patient liability
¥
¥
First/subsequent visit fees Admission charges, etc.
Diagnostic procedure
combination (DPC)
Medical supervision charges, etc. Home medical care
Insurance points
Patient liability
¥ ¥ ¥ ¥ ¥
Examinations Diagnostic imaging Medication Injections Rehabilitation
Insurance points
Patient liability
¥ ¥ ¥ ¥ ¥
Specialized psychiatric treatment Medical treatment Surgery Blood transfusion Anesthesia
Insurance points
Patient liability
¥ ¥ ¥ ¥ ¥
Radiotherapy Pathological diagnosis
Dental crown restoration /
Prosthodontics
Prescriptions SUBTOTAL
Insurance points
Patient liability
¥ ¥ ¥ ¥
¥
医療費領収書 : 2014 年3月初版