HTML Preview Doctors Medical Receipt page number 1.
MEDICAL SUPPLY
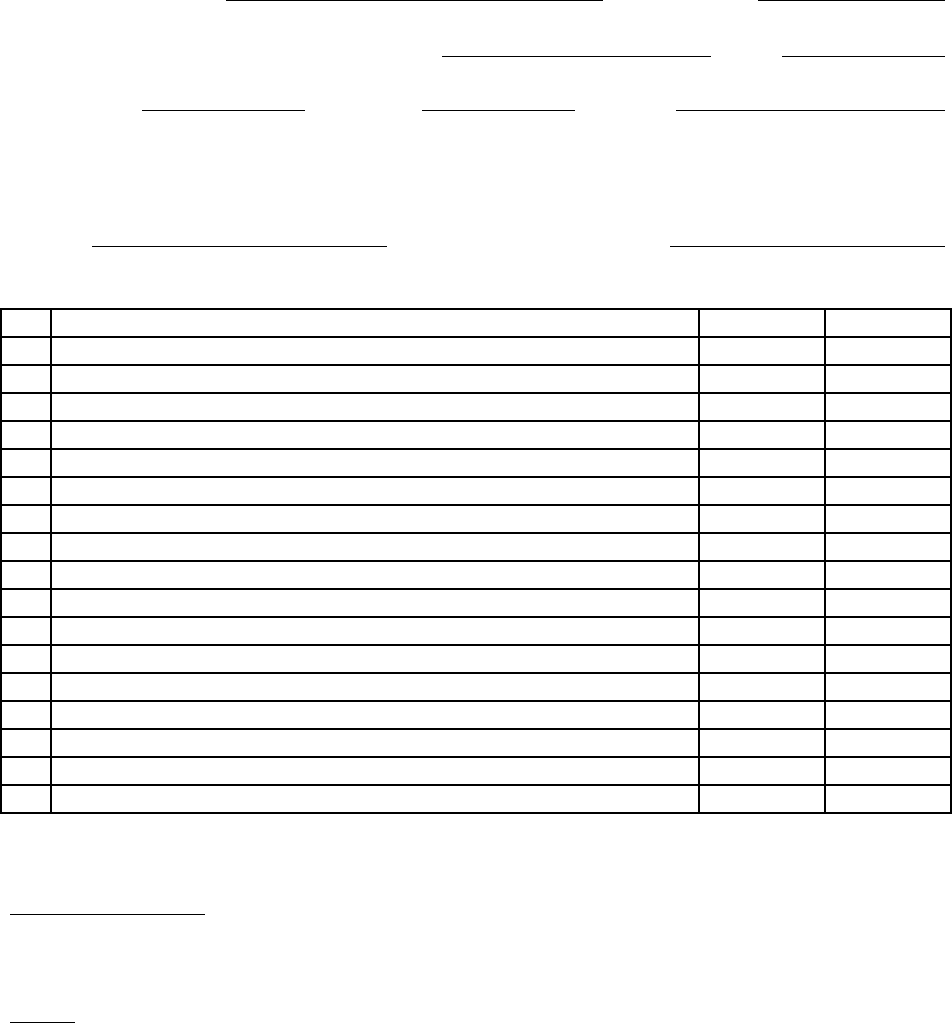
RECEIPT AND INVENTORY FORM
INCIDENT NAME: INCIDENT #:
A. Supplies/Equipment received from: DATE: / /
Agency:
Unit ID#:
Name:
(Whenever possible, use masking tape and markers to identify all equipment)
B. Supplies/Equipment Received by:
NAME:
INCIDENT POSITION:
No. Item Description (Print All Entries) Unit* Amount
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
*Unit - list a measurable description of the item (gauge, gm, ml, bag, doz., etc.)
Form distribution: (Use carbon paper) Original - Medical Supply Coordinator
Copy - Source of Supply
INCIDENT RE-IMBURSEMENT OF ANY SUPPLIES/EQUIPMENT WILL BE BASED
ONLY UPON ORIGINAL FORM LISTINGS.
I-MC-312 (1/8/92)