HTML Preview Motor Vehicle Weekly Safety Checklist page number 1.
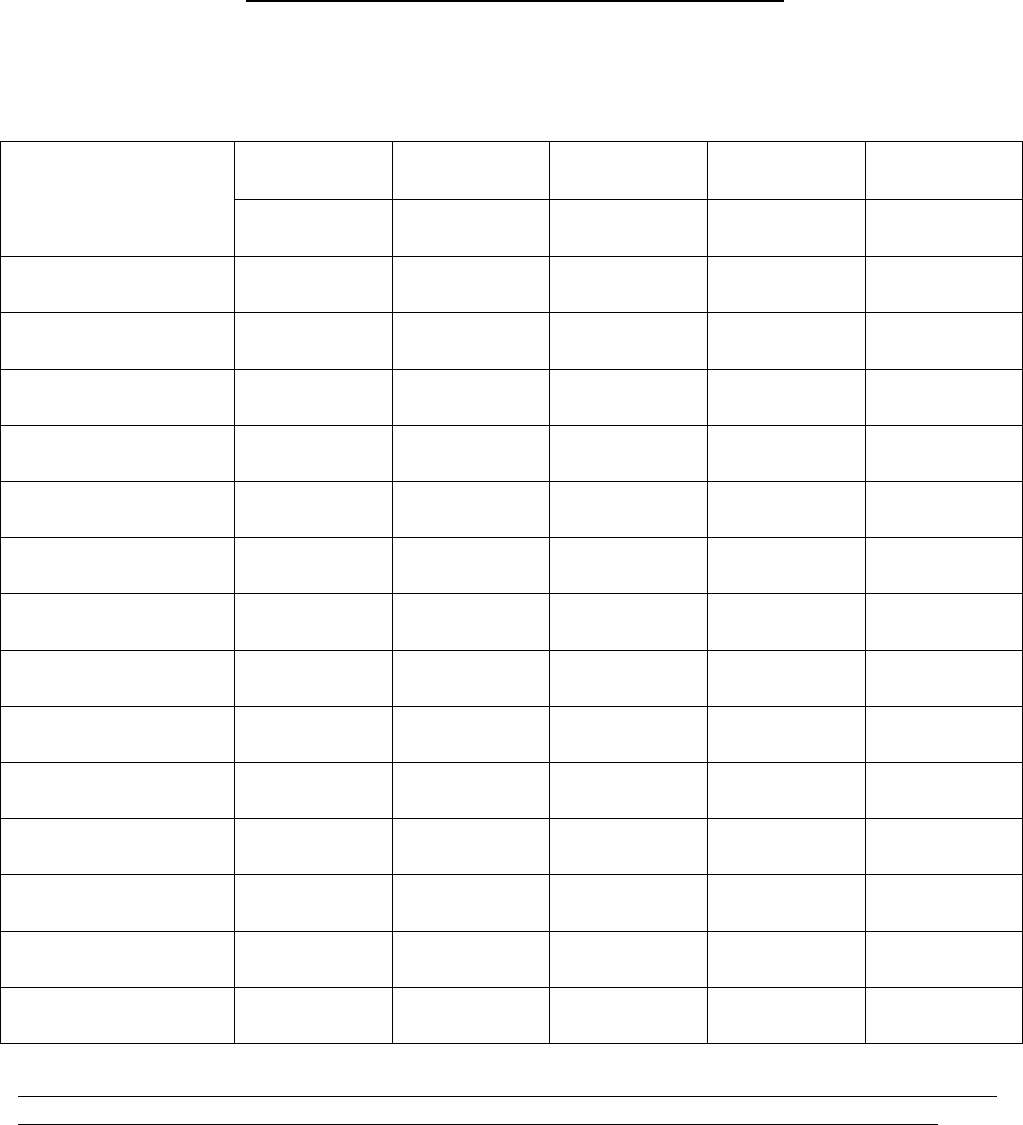
MOTOR VEHICLE WEEKLY SAFETY CHECKLIST
Department: ____________________
Vehicle Make: ______________ Model: ________________ V.I.N.#__________________________
Do not operate any
vehicle if an unsafe
condition exists.
Inspection Date:
/ /
Inspection Date:
/ /
Inspection Date:
/ /
Inspection Date:
/ /
Inspection Date:
/ /
Inspected By: Inspected By: Inspected By: Inspected By: Inspected By:
Windshield wipers
and washers
Directional Signals
Lights
Horn and Mirrors
Inspection sticker
current
Tag current
Check for 4000 mile
maintenance
Tire inflation and safe
tread depth
Power steering fluid
Antifreeze / Coolant
Motor oil level
Brake fluid &
Brake operation
Exterior and Interior
condition acceptable
Transmission Fluid &
Hydraulics (if applic.)
Any item not passing inspection shall immediately be brought to the attention of the department head,
a garage work order issued, and the vehicle repaired and returned to service as soon as possible.
Comments: ________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
***SUBMIT CHECKLIST TO HUMAN RESOURCES ON THE 5
TH
DAY OF EACH MONTH***
Revised 8-06-08 BG