HTML Preview Child Asthma Management Plan page number 1.
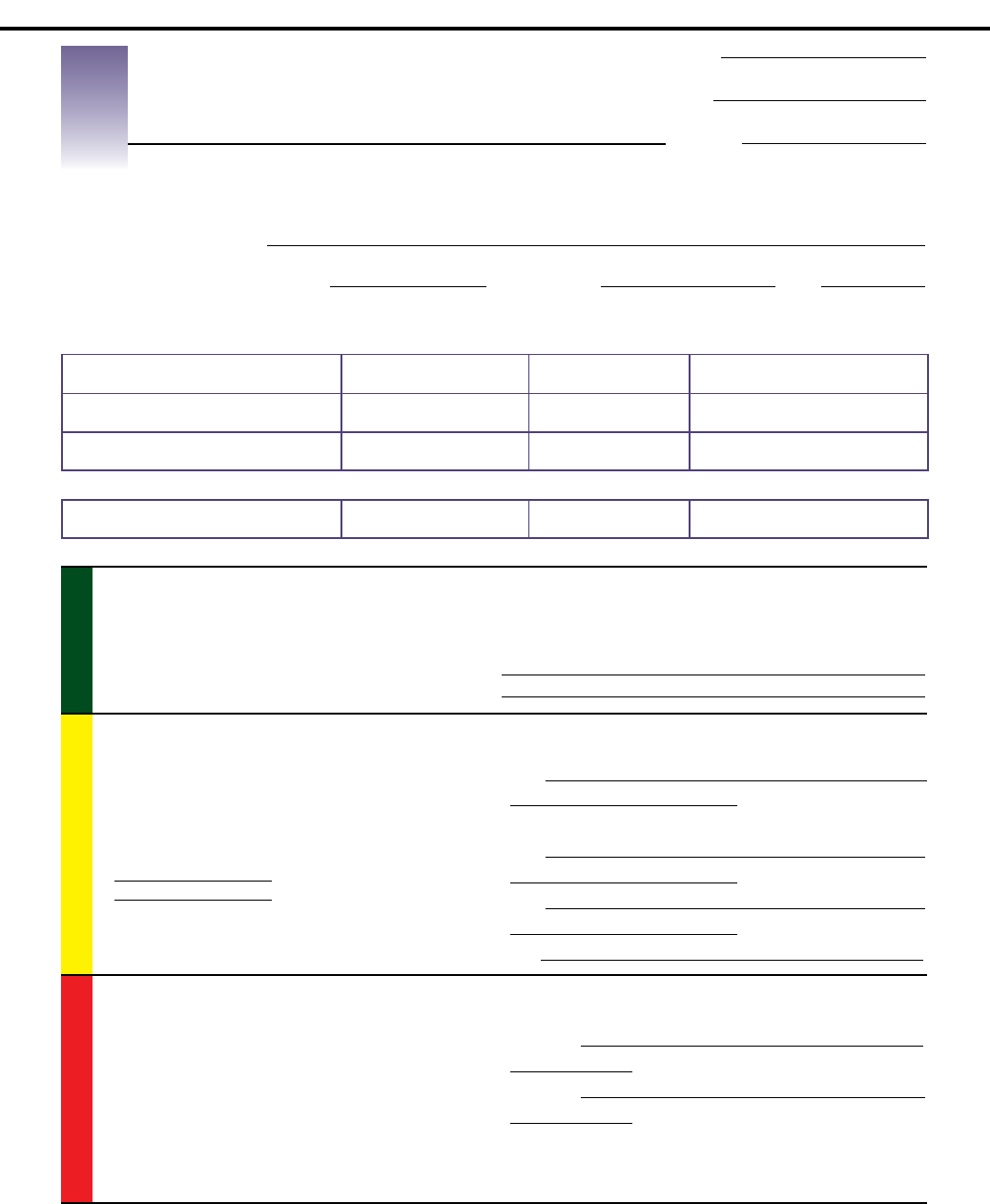
SAMPLE ASTHMA ACTION PLAN
Asthma Action Plan,
for Children 0–5 Years
Health Care Provider’s Name
Health Care Provider’s Phone Number Completed by Date
Long-Term Control Medicines
(Use every day to stay healthy) How Much To Take How Often
Other Instructions
(such as spacers/masks, nebulizers
_____ times per day
EVERY DAY
_____ times per day
EVERY DAY
_____ times per day
EVERY DAY
Quick-Relief Medicines How Much To Take How Often Other Instructions
Give ONLY as needed
NOTE: If this medicine is needed often
( _____ per week), call physician
GREEN ZONE
Child is WELL and has no asthma symptoms,
even during active play
Prevent asthma symptoms every day
• Give the above long-term control medicines every day
• Avoid things that make the child’s asthma worse
Avoid tobacco smoke, ask people to smoke outside
YELLOW ZONE
Child is NOT WELL and has asthma symptoms that
may incude:
• Coughing
• Wheezing
• Runny nose or other cold symptoms
• Breathing harder or faster
• Awakening due to coughing or difficulty breating
• Playing less than usual
•
•
Other symptoms that could indicate that your child is having
trouble breathing may include: difficulty feeding (grunting
sounds, poor sucking), changes in sleep patterns, cranky and
tired, decreased appetite
CAUTION: Take action by continuing to give regular asthma medicines
every day AND:
Give
(include dose and frequency)
If the Child is not in the Green Zone and still has symptoms after 1 hour:
Give
(include dose and frequency)
Give
(include dose and frequency)
Call
RED ZONE
Child FEELS AWFUL warning signs may incude:
• Child’s wheeze, cough or difficult breathing continues
or worsens, even after giving yellow zone medicines
• Child’s breathing is so hard that he/she is having
trouble walking/talking/eating/playing
• Child is drowsy or less alert than normal
DANGER!
MEDICAL ALERT! Get help!
Take the child to the hospital or call 9-1-1 immediately!
Give more
(include dose and frequency) until you get help
Give more
(include dose and frequency) until you get help
Get help immediately! Call 9-1-1 if: • The child’s skin is sucked in around neck and ribs or
• Lips and/or fingernails are grey or blue, or
• Child doesn't respond to you.
Name
DOB
Record #
Source: http://www.calasthma.org/uploads/resources/actionplanpdf.pdf. San Francisco Bay Area Regional Asthma Management Plan.
http://www.rampasthma.org
Source: National Heart, Lung, and Blood Institute National Asthma Education and Prevention. Expert Panel Report 3; Guidelines for the Diagnosis
and Management of Asthma; Full Report 2007. Bethesda, MD: NHLBI; 2007:118.