HTML Preview Patient Progress Note page number 1.
Patient Progress Note
Please fill out form at each visit and return to the front desk assistant when finished. Thank you for your assistance.
Patient Name ___________________________________________ Date_____________________
Please mark the level of intensity of your symptoms using the following scale.
(0 equals no symptom at all, 100 equals maximum possible intensity of the symptom.)
Symptom___________________________________ 0 10 20 30 40 50 60 70 80 90 100
Symptom___________________________________ 0 10 20 30 40 50 60 70 80 90 100
Symptom___________________________________ 0 10 20 30 40 50 60 70 80 90 100
Symptom___________________________________ 0 10 20 30 40 50 60 70 80 90 100
Please rate by circling your overall state of wellness since your last treatment
Significantly Improved Improved Unchanged Worsened Significantly Worsened
(Office Use Only) PATIENT’S NOTES
Units:
Set: 1 2 3 4
Needle #
LV
GB
HT
SI
PC
SJ
SP
ST
LU
LI
KD
UB
REN
DU
EXTRA
ASHI
SCALP
EAR
MOXA/TDP
TUINA/CUP
o (Check here if documenting any physician notes on reverse) Physician’s Signature:________________________
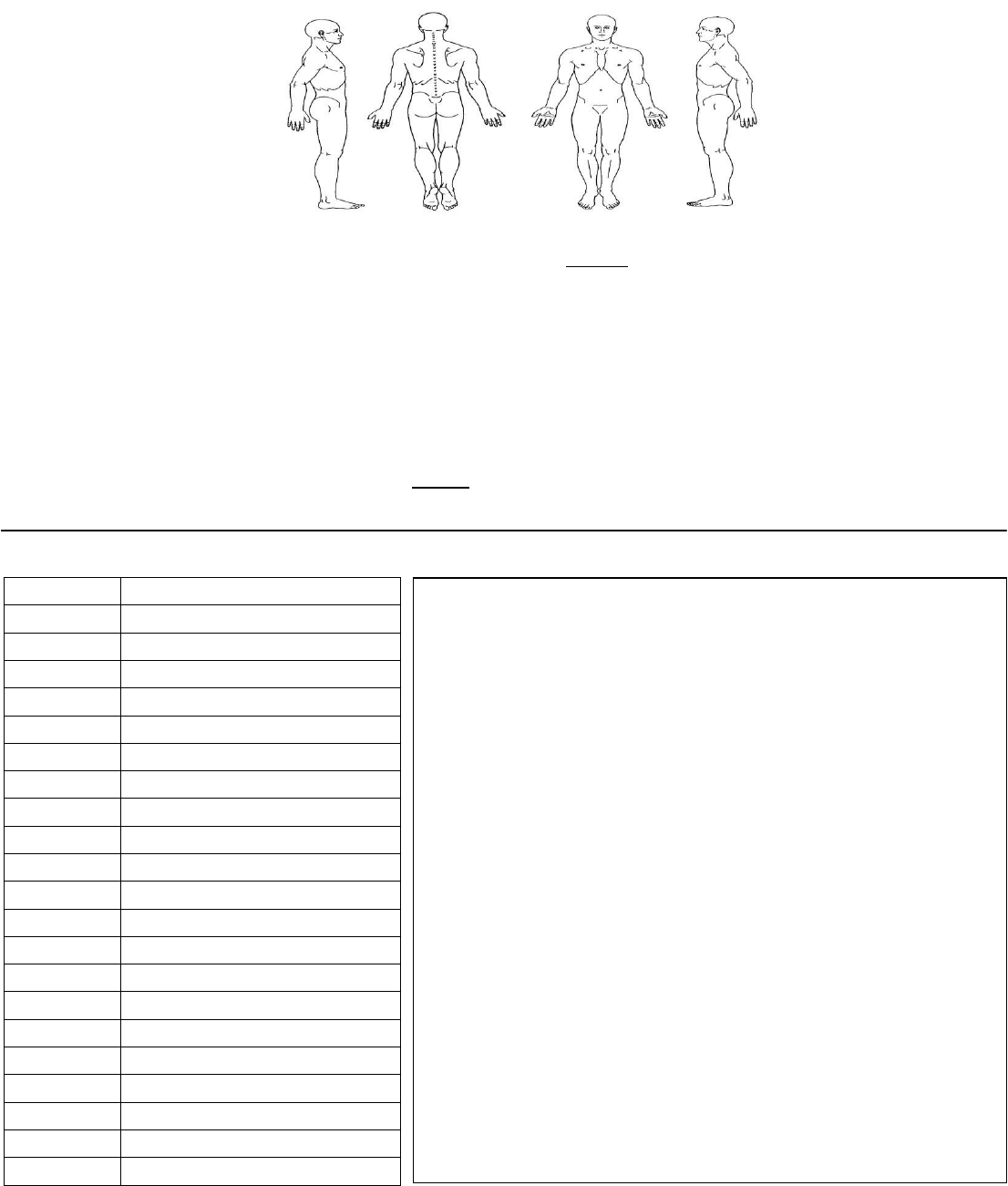
Please mark the area
where there is pain.
X=Sharp Pain
O=Dull Pain
What has changed?
________________________________________________________
________________________________________________________
________________________________________________________
________________________________________________________
Do you have any health concerns that you would like to
communicate to the doctor other than those for which you are
currently being treated for? If yes, please describe:
________________________________________________________
________________________________________________________
________________________________________________________
________________________________________________________
________________________________________________________